
A University of Auckland professor’s work has led to the development of a vital new tool for medical staff caring for patients hospitalised with serious COVID-related illness.
At the beginning of the year, there were 118 million people infected worldwide. Of these, about 5% became critically ill and were admitted to intensive care units. That adds up to about six million intensive care beds required over the previous 12 months.
The majority of these six million desperately ill patients have required mechanical ventilators to breathe while their immune systems fought back against the virus. In Brazil, Italy, the United States and other countries, medical teams have had to decide who among their patients should receive the benefit of the limited numbers of ventilators and who should not.
Intensive care teams rely on a set of physiological signals, from electrocardiograms, oxygen saturation, carbon dioxide levels and the flow of respiration to monitor and determine those patients who need to be on a ventilator and to guide care and treatment once ventilation starts.
Professor Merryn Tawhai (pictured) of the Auckland Bioengineering Institute is an engineer who collaborates with clinicians, including intensive care specialists.
“One of the major issues when facing shortages of mechanical ventilators is determining who will most benefit,” said Professor Tawhai.
“So, if you’re faced with two patients with the same physiological signals, both on non-invasive ventilation, how do you make a decision about who needs mechanical ventilation? That’s a terrible dilemma for clinical staff and their patients in intensive care units.”
Difficult decisions
“At an international level New Zealand intensive care physicians have an excellent reputation,” Prof Tawhai says.
“They do a fantastic job.”
And New Zealand physicians will be thankful to have not been forced to make the difficult decision to ration ventilators.
But whether they practise in New Zealand or overseas, intensive care physicians deploy the same mix of skill, knowledge and experience.
Yet, as Prof Tawhai says, “In some respects, they’re managing people almost blindly because most of the monitoring data available is to an extent after the fact”.
The readouts let the physician build a mental picture of a patient’s lungs, but the information is not based on direct observation of the lungs.
“There could be a lot of change going on inside the lung that takes a while to reveal itself,” she said.
“A patient might be developing damage due to systemic inflammation, there might be leakage from blood vessels that in turn leads to pulmonary edema (excess fluid in the lungs that can be life threatening) that makes the lung ‘stiff’ and ‘heavy’.
“There actually has to be quite a bit of damage to the lung before it will be obvious on clinical data.”
There are further risks for patients on ventilation because the intensive care team is trying to find the sweet spot, where the machine provides enough pressure to keep airways open to receive enough air while taking care to not over inflate the lungs and stretch delicate tissue. This has the potential to cause damage.
Prof Tawhai says, “The diagnostic information they can get is not precise enough to figure out what’s exactly happening”.
This is the perennial challenge for critically ill and sedated patients. They are often too ill to move for an MRI or CT scan, while the very act of moving Covid patients within hospitals breaches infection control protocols. The experience of the physician becomes paramount. They tweak treatments, adjust ventilator settings, prescribing drugs and wait for improvement.
With high numbers of patients on ventilators there is a corresponding rise in ventilator induced lung injury and acute respiratory distress syndrome (ARDS). Reviews suggest that ARDS caused by Covid exacts a higher death toll than other causes of the syndrome with a mortality rate of between 65 and 94% for COVID-19 patients. Survivors risk permanent lung damage and difficulty breathing for the rest of their lives.
Prof Tawhai has a unique perspective on this global problem. For 20 years she has led work on a digital human lung model, a key part of the ambitious human Physiome project at the Auckland Bioengineering Institute to create computer models of human physiology that accurately mirror organs in real time. A digital rendition of a heart or lung can be used to safely test new treatments.
Doctors need a way to look directly at their critically ill patient’s lungs. If they could see what was happening, the parts of the lung in distress, the degree the tissue was stiffening and where the shadows of pneumonia were forming, along with other factors, they could make treatment decisions earlier and with more confidence. The answer Prof Tawhai has come up with combines an existing technique, Electrical Impedance Tomography (EIT), with biophysical modelling from the lung Physiome project to create a life-like three-dimensional model of an intensive care patient’s lungs.
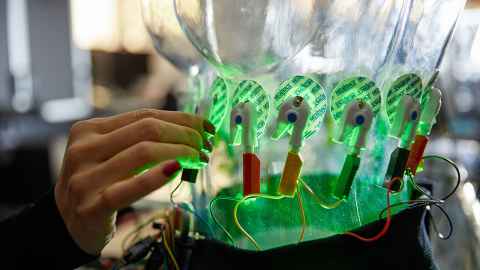
Electrical Impedance Tomography is a non-invasive way to deliver medical imagery. The images are built up by placing electrodes around a patient’s body. By running a low current through a series of electrodes taped to a patient, EIT measures the difference in conductivity between different parts of anatomy, for example, bone and tissue and the air in the lungs. From the differences, EIT devices construct an image of the internal organs and systems.
However, Prof Tawhai says there has been relatively low uptake of EIT imaging by clinicians. Interpreting information from EIT is not straightforward and the method has low resolution compared with other imaging techniques, therefore its cost currently outweighs its benefit. With $495,000 of COVID-19 capability funding from the Government, Prof Tawhai and her team have brought together existing technologies and expertise to create a non-invasive way to monitor what’s happening in a critical care patient’s lungs.
They have developed a very low cost EIT device that they have merged with detailed models of lung structure. They plan to leverage machine learning methods to improve image reconstruction, and link the imaging data to other clinical data via their biophysical models. If it succeeds it will be like looking through a transparent torso, at lungs struggling against the virus and its impact.

“This all fits together really well,” Prof Tawhai says.
“We have developed our models of the lung and its sub-structures, the ventilation and perfusion, gas exchange and tissue mechanics.”
The lung model the team has compiled includes a broad range of ages, heights, weights and ethnicities. And better still, once the prototype passes testing, the potential for rapid commercialisation and scale means that the technology will build ever more refined models from the leap in data coming in from critical care units.
One day, she envisages New Zealand intensive care units using model-based EIT as a matter of course to assist with patient management. Despite centuries of medical research, our bodies continue to hold mysteries.
As an engineer, Prof Tawhai says she is at the right place. “What we’re doing requires expertise in solid mechanics, fluid mechanics, software engineering, and electrical engineering, as well as a thorough understanding of lung physiology”.
The lung imaging project brings together multiple, intersecting and overlapping layers of complexity with clinical practice and leading-edge science.
Story by Gilbert Wong for the University of Auckland.

